What is Femoroacetabular Impingement and what causes it?
Femoroacetabular refers to the place where the femur (thigh bone) and acetabulum (hip socket) meet. Impingement means pinching.In the case of femoroacetabular impingement (FAI), the head of the femur butts up against the cartilage and pinches it. Normally, the femoral head moves smoothly inside the hip socket. The socket is just the right size to hold the head in place.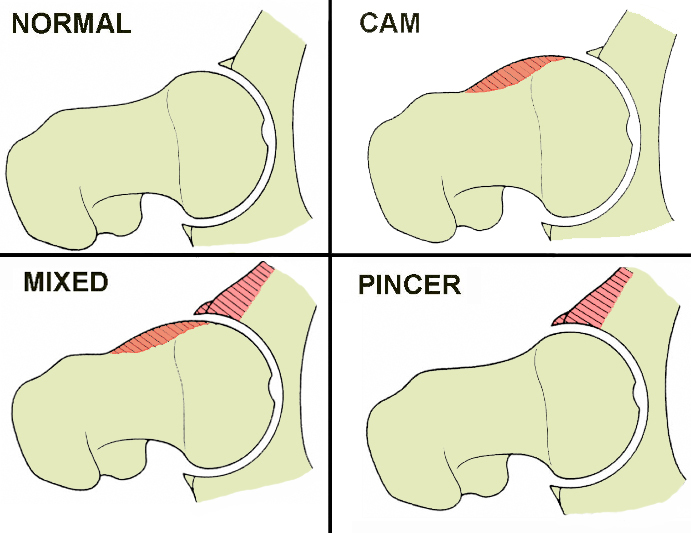 If the acetabulum is too shallow or too small, the hip can dislocate. In the case of FAI, the socket may be too deep. The rim of the cartilage hangs too far over the head. When the femur flexes and rotates, the cartilage gets pinched. This causes deep groin pain with activities that stress hip motion. Prolonged walking is especially difficult. The cause of the problem is under considerable debate. For a long time it was assumed that overload of the joint caused this kind of OA. But no one could identify what was causing the stress overload. Now with better imaging studies, we know that some subtle changes in the shape of the femoral head may be the cause of FAI. Other anatomical changes in the angle of the hip may also contribute to this problem. And as mentioned, FAI can occur if the hip socket is too deep. If the acetabulum is too shallow or too small, the hip can dislocate. In the case of FAI, the socket may be too deep. The rim of the cartilage hangs too far over the head. When the femur flexes and rotates, the cartilage gets pinched. This causes deep groin pain with activities that stress hip motion. Prolonged walking is especially difficult. The cause of the problem is under considerable debate. For a long time it was assumed that overload of the joint caused this kind of OA. But no one could identify what was causing the stress overload. Now with better imaging studies, we know that some subtle changes in the shape of the femoral head may be the cause of FAI. Other anatomical changes in the angle of the hip may also contribute to this problem. And as mentioned, FAI can occur if the hip socket is too deep.
Preliminary Results of Labral Refixation Norman Espinosa, MD1, Dominique A. Rothenfluh, MD2, Martin Beck, MD2, Reinhold Ganz, MD1 and Michael Leunig, MD3 1 Department of Orthopaedics, Background: Recent advances in the understanding of the anatomy and function of the acetabular labrum suggest that it is important for normal joint function. We found no available data regarding whether labral refixation after treatment of femoro-acetabular impingement affects the clinical and radiographic results. Methods: We retrospectively reviewed the clinical and radiographic results of fifty-two patients (sixty hips) with femoro-acetabular impingement who underwent arthrotomy and surgical dislocation of the hip to allow trimming of the acetabular rim and femoral osteochondroplasty. In the first twenty-five hips, the torn labrum was resected (Group 1); in the next thirty-five hips, the intact portion of the labrum was reattached to the acetabular rim (Group 2). At one and two years postoperatively, the Merle d'Aubigné clinical score and the Tönnis arthrosis classification system were used to compare the two groups. Results: At one year postoperatively, both groups showed a significant improvement in their clinical scores (mainly pain reduction) compared with their preoperative values (p = 0.0003 for Group 1 and p < 0.0001 for Group 2). At two years postoperatively, 28% of the hips in Group 1 (labral resection) had an excellent result, 48% had a good result, 20% had a moderate result, and 4% had a poor result. In contrast, in Group 2 (labral reattachment), 80% of the hips had an excellent result, 14% had a good result, and 6% had a moderate result. Comparison of the clinical scores between the two groups revealed significantly better outcomes for Group 2 at one year (p = 0.0001) and at two years (p = 0.01). Radiographic signs of osteoarthritis were significantly more prevalent in Group 1 than in Group 2 at one year (p = 0.02) and at two years (p = 0.009). Conclusions: Patients treated with labral refixation recovered earlier and had superior clinical and radiographic results when compared with patients who had undergone resection of a torn labrum. Although the results must be considered preliminary, we now recommend refixation of the intact portion of the labrum after trimming of the acetabular rim during surgical treatment of femoro-acetabular impingement. Level of Evidence: Therapeutic Level III. See Instructions to Authors for a complete description of levels of evidence. For complete article click here Updated February 2009 |